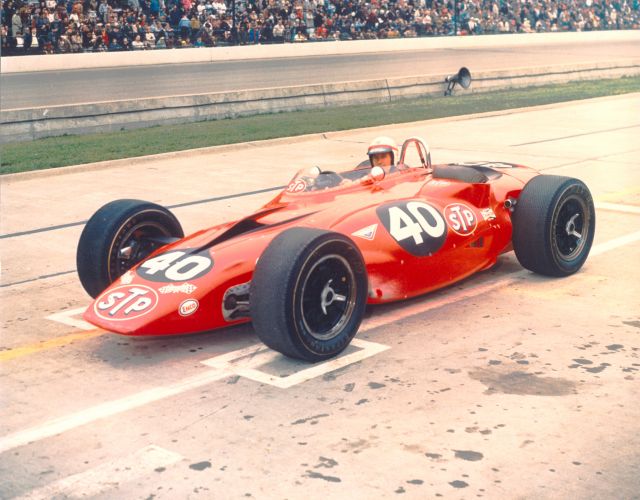
There are a thousand examples that could be used to show the rot caused by the invidious tenets of socialism in our sports these days. The most illustrative, in my opinion, is that of IndyCar. For the first 75 years of the Indianapolis 500, the race and the supporting series were based on a free-market-style “run what you brung” model, resulting in a rich and storied tradition. Stories of turbine cars, diesels, close finishes, and 1000 HP rocketships on wheels echo through from the past. Before NASCAR, the various iterations of Indycar (CART, USAC, AAA, etc.) were king in the United States. Until the late 90s, IndyCar was a half-step behind Formula 1 for international popularity.
years of the Indianapolis 500, the race and the supporting series were based on a free-market-style “run what you brung” model, resulting in a rich and storied tradition. Stories of turbine cars, diesels, close finishes, and 1000 HP rocketships on wheels echo through from the past. Before NASCAR, the various iterations of Indycar (CART, USAC, AAA, etc.) were king in the United States. Until the late 90s, IndyCar was a half-step behind Formula 1 for international popularity.
Today, IndyCar is circling the drain. They had a race in Phoenix last weekend with 7,000 attendees and a few hundred thousand, at most, watching on TV. Why such a precipitous drop from rivaling F1 to now being on the brink of failure? Beyond the basic ineptitude and competitive failures that doom any venture, the problem can be summed up in one word: socialism.
In the early 90s, CART (as IndyCar was called at the time) was king. Names like Unser, Andretti, and Foyt were touring North America, racing custom built race cars in front of packed stands. The Indy 500 would have 350k+ on hand for the annual culmination of a monthslong celebration of speed. Most years, certain qualifying days would have well over 100k people on hand. In 1994, the fastest qualifying speed was a hair over 228 MPH. Today, almost 25 years later, the cars do the same speed, the crowds are down and the hallowed Month of May has become a week and a half.
Then, in response to escalating costs and a perceived shift away from the small-town American dirt track racers to foreign racers in the F1 minor leagues, the owners of the Indianapolis Motor Speedway started the IRL, which based its operating model on a top-down financing of the racing efforts of smaller teams. There are a bunch of other factors in the decadal decline of IndyCar, including a split into two series, series-wide emphasis on safety over speed, and the rise of NASCAR, but the biggest factor was the susceptibility to the allure of socialism.
In the attempt to contain costs and attract smaller teams, the IRL and, later, IndyCar continued with two core principles that will sound familiar to all of you who are versed in the language of the socialist. First, IndyCar established a phonebook’s worth of technical regulations meant to curtail engineering costs. This resulted in the last 10+ years being run with a single allowable chassis each year. They have allowed limited competition in the engine, suspension, and aerodynamics, but the days of building your own mousetrap are over. Second, IndyCar established what’s called the “Leader’s Circle,” which is an alternative to the traditional purse system. Instead of the winner getting a zillion dollars and last place going home with a pittance, anybody who runs a certain percentage of the annual schedule is paid a salary for each full-time race car run, and winners are given a nominal sum as a prize.
 As can be easily predicted by those of us familiar with the stories of Soviet Russia, Venezuela, Cuba, and North Korea, IndyCar has been suffering from poor racing, fewer teams, fewer race cars, and an utter collapse of the fanbase. Besides a single day per year burning off 75 years of tradition, American Open-Wheel Racing is on life support. Of course, these are “bad economic times” and “motorsports is on a decline” and “we can’t afford competition.” The excuses have been flying since 1996 when they first headed down this path. Every half-hearted, feeble attempt to introduce a market influence is quickly undone. The toe in the water is withdrawn as soon as they realize it’s wet.
As can be easily predicted by those of us familiar with the stories of Soviet Russia, Venezuela, Cuba, and North Korea, IndyCar has been suffering from poor racing, fewer teams, fewer race cars, and an utter collapse of the fanbase. Besides a single day per year burning off 75 years of tradition, American Open-Wheel Racing is on life support. Of course, these are “bad economic times” and “motorsports is on a decline” and “we can’t afford competition.” The excuses have been flying since 1996 when they first headed down this path. Every half-hearted, feeble attempt to introduce a market influence is quickly undone. The toe in the water is withdrawn as soon as they realize it’s wet.
The path to success is simple and quite obvious. Undoing 25 years of stupid will hurt, but, as Venezuela is figuring out right now, the pain is inevitable. IndyCar will wither into nothing unless it reintroduces the competitive spirit of the free market into the sport. The excuses of the boot-lickers in the sport are all based on some nugget of truth, but IndyCar isn’t failing because motorsports are unpopular or because the economy is bad. IndyCar is failing because socialism is more than just painful to live under, it’s also painful to watch.
It’s sad to see such a great tradition go down in flame, but these days even our sports act as a cautionary tale against socialism and all its variants.